¹University of Alberta, Edmonton, Canada, ² Alberta Retina Consultants, Edmonton, Canada
A 70-year-old male was referred for assessment of bilateral asymptomatic hypopigmented chorioretinal lesions. His ophthalmic history was significant for previous retrobulbar optic neuritis in the right eye. Medical history was significant for previous cerebrovascular accident.
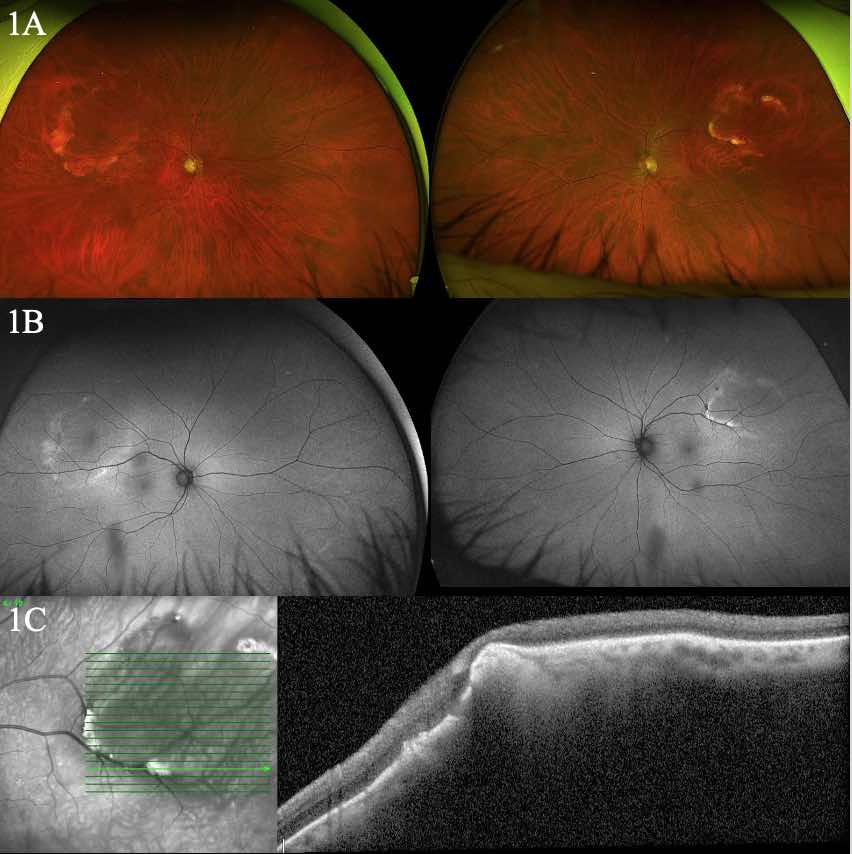
On examination visual acuity was 20/30 OD and 20/25 OS. Intraocular pressures were within normal limits. Anterior segment examination was unremarkable OU. Posterior examination revealed elevated amelanotic lesions in the supratemporal retinal quadrant in both eyes (Fig 1A). There was no associated subretinal fluid. Autofluorescence revealed hyperautofluorescence at the edge of the lesions (Fig 1B). OCT over the lesions was performed that identified sclerochoroidal elevation (Fig 1C). B scan ultrasound was then performed which revealed a hyperechoic signal with shadowing in keeping with calcification. The diagnosis of bilateral sclerochoroidal calcification was made.
Sclerochoroidal calcifications are benign calcific deposits on the differential for amelanotic choroidal lesions. On histology these lesions show calcium pyrophosphate deposition in the sclera and choroid. They are classically located in the supertemporal or superonasal quadrants of the retina.1 Four patterns of appearance have been described by Hasanreisoglu et al. utilizing enhanced depth OCT. The described patterns include “flat”, “rolling”, “rocky-rolling”, or “table mountain” with the “rocky-rolling” being most characteristic for sclerochoroidal calcifications.2 A hyperechoic lesion is typical on ultrasound representing the calcification. These lesions are most commonly benign with rare associations to recurrent inflammation or disorders of calcium metabolism.1 Choroidal neovascularization is a rare complication of these lesions.3 Identification of sclerochoroidal calcification is important as it can mimic more concerning etiologies such as amelanotic melanoma and metastatic lesions.
Figures
Figure 1: Optos pseudocolor photo of both eyes with superotemporal sclerochoroidal calcification present (A). Autofluorescence images of both eyes corresponding to pseudocolor image (B). Spectralis OCT (Heidelberg) through the sclerochoroidal calcification in the left eye.
References
1. Thomson AC, Brown GT, Dolores-Rodriguez A, Hunter AA. A Case of Extensive Bilateral Idiopathic Sclerochoroidal Calcification and Review of Literature. Int Med Case Rep J. 2021;14:749-755. doi:10.2147/IMCRJ.S336237
2. Hasanreisoglu M, Saktanasate J, Shields PW, Shields CL. CLASSIFICATION OF SCLEROCHOROIDAL CALCIFICATION BASED ON ENHANCED DEPTH IMAGING OPTICAL COHERENCE TOMOGRAPHY “MOUNTAIN-LIKE” FEATURES. Retina. 2015;35(7):1407-1414. doi:10.1097/IAE.0000000000000468
3. Goerlitz-Jessen M, Ali MH, Grewal DS. Rare Complication of Sclerochoroidal Calcifications. JAMA Ophthalmol. 2019;137(1):111-112. doi:10.1001/jamaophthalmol.2018.2457