Illinois Eye and Ear Infirmary; Department of Ophthalmology and Visual Sciences, University of Illinois at Chicago
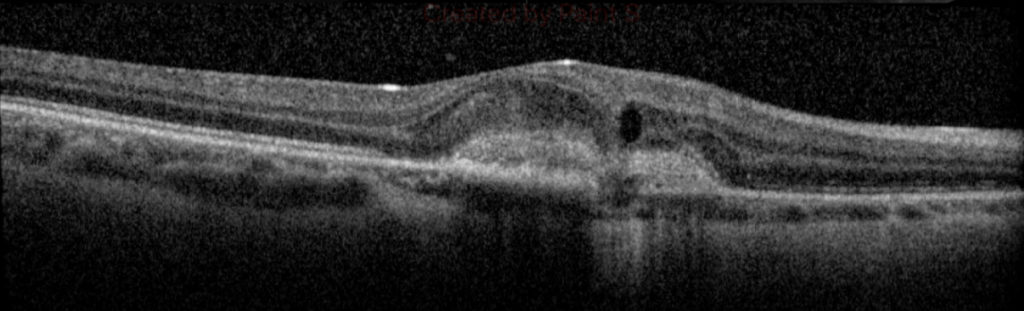
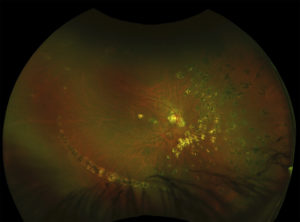
A 26-year-old healthy Hispanic-American female who grew up in the Ohio Mississippi River Valley presented with a two-month history of decreased vision involving the right eye described as a stationary “central spot”. Her past ocular history was significant for myopia OU. On examination, visual acuity with correction was count fingers at 3 feet OD and 20/40 OS. Fundus examination OU showed no vitreous cell or haze with tilted optic nerves and peripapillary atrophy. Fundus exam was significant for wide-spread chorioretinal scarring OD (Figure 1). Retinal findings were purely unilateral. Fluorescein angiography demonstrated staining of the multifocal scars scattered throughout the fundus with leakage from the juxtafoveal scar concerning for an active choroidal neovascular membrane (CNVM). Optical coherence tomography (OCT) showed subretinal hyperreflective material with intraretinal fluid OD (Figure 2).
The patient was diagnosed with Presumed Ocular Histoplasmosis (POHS) complicated by a CNVM. POHS is theorized to be an immune response to the yeast variant of Histoplasma capsulatum, which predominates along the Ohio and Mississippi River Valleys1. Patients tend to be asymptomatic unless a CNVM develops, which is found in approximately 3.8% of patients with POHS-related chorioretinal scarring2. Patients are traditionally observed unless a vision threatening CNVM develops3.
The patient received an intra-vitreal bevacizumab injection OD. Four weeks later, vision was unchanged with development of a serous pigment epithelial detachment (PED) in association with the prior observed fibrovascular CNVM. Further injections were not recommended as the visual gain was minimal due to chronicity of the CNVM given the fibrotic response. At recent examination, one-year post-presentation, there was minimal coalescence of the fibrovascular CNVM and PED, and vision has remained stable.
1 Diaz RI, Sigler EJ, Rafieetary MR, et al. Ocular histoplasmosis syndrome. Surv Ophthalmol. 2015; 60(4): 279-95.
2 Lewis ML, Van Newkirk MR, Gass JD. Follow-up study of presumed ocular histoplasmosis syndrome. Ophthalmology. 1980; 87(5): 390-9.
3 Nielsen JS, Fick TA, Saggau DD, et al. Intravitreal anti-vascular endothelial growth factor therapy for choroidal neovascularization secondary to ocular histoplasmosis syndrome. Retina. 2012; 32: 468-72.